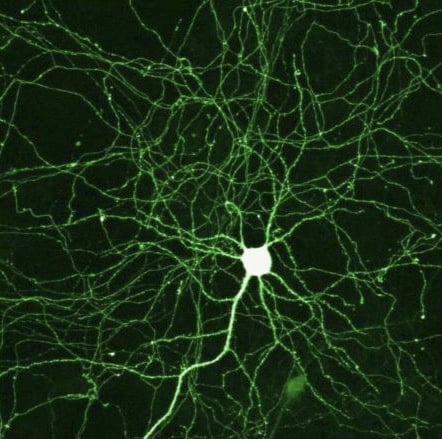
Stem cell researchers have been exploring ways of converting human body cells into neural cells specific to dopamine, an important chemical in the brain. Now it seems they may have found one mix of factors that stimulates this conversion directly. It is hoped that one day such cells may be suitable to replace neurons lost through neurodegeneration in Parkinson’s disease (PD).
Dopamine pathways in the brain. In Parkinson’s disease, the substantia nigra degenerates, affecting the striatum, which controls normal motor function.
PD is becoming a growing threat to today’s aging population, with 127,000 people living with this disease in the UK alone. Characterised by the progressive deterioration of dopamine neurons in an area of the brain called the substantia nigra, patients with PD suffer from debilitating movement difficulties that worsen over time. With no cure known and only a few drugs- e.g. levadopa, a dopamine source – to manage patient symptoms, stem cell research has offered a promising new platform towards finding an effective PD treatment.
Numerous studies so far have shown successful generation of dopamine neurons by reprogramming existing donor cells, using specific proteins called transcription factors. When transplanted into rodent and primate models of Parkinson’s disease, these neurons can help alleviate symptoms.
Unfortunately, the two donor cell types suggested for cell conversion until now face various issues. Embryonic stem cell (ESC) use is ethically controversial, while manipulating mature cells- for instance, fibroblasts – to dedifferentiate first to become induced pluripotent stem cells (iPSCs) is time consuming and expensive.
One potential solution? – Cut out the middle men (the iPSCs).
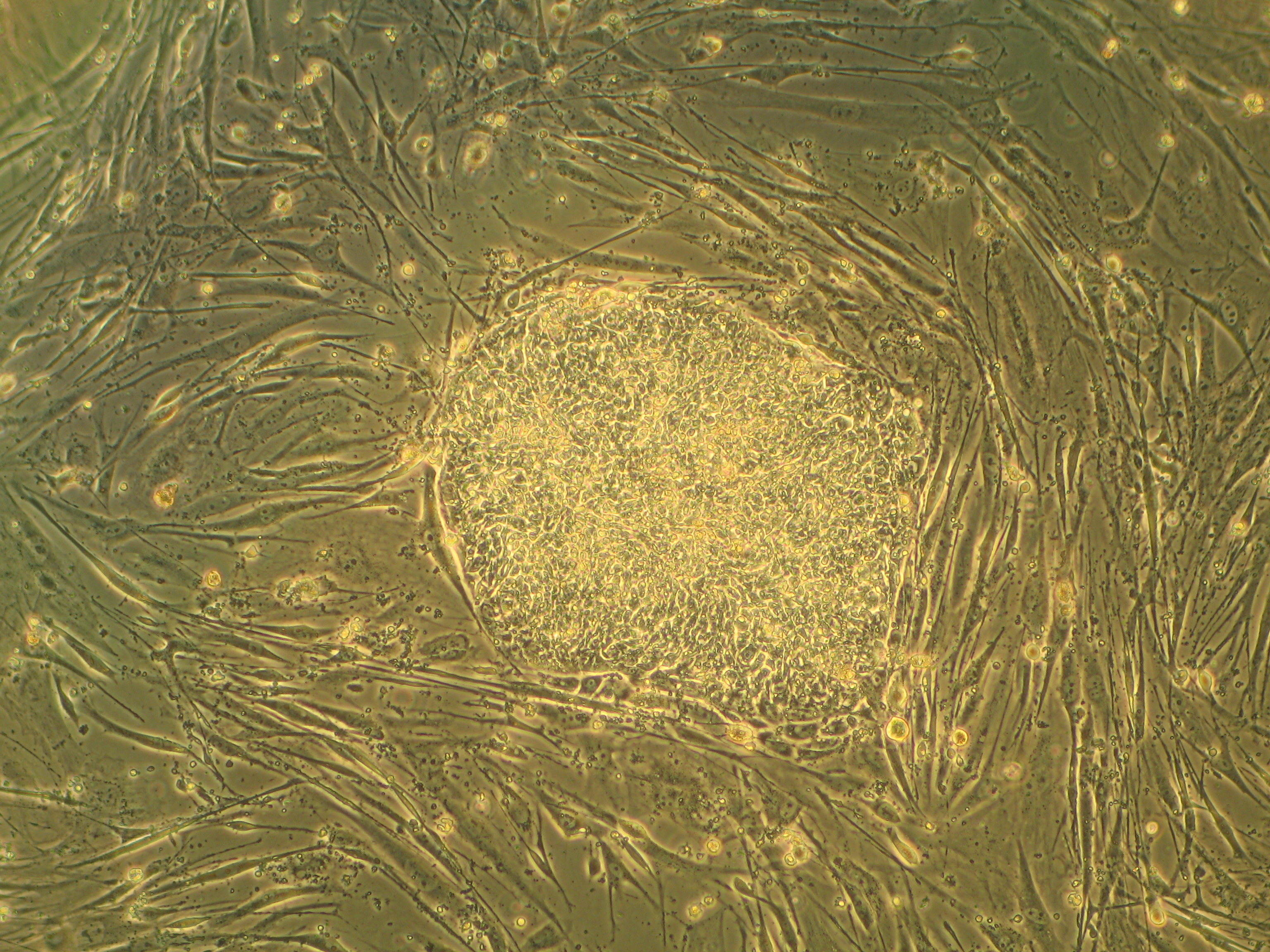
A colony of embryonic stem cells. The cells in the background are mouse fibroblasts cells. (NIH image)
Xinjian Liu and his team at the Radiation Oncology department at Colorado University, have been working to generate dopamine neurons directly from human fibroblasts, without producing iPSCs first. And it seems they may have identified a suitable combination of transcription factors that makes this happen.
Liu’s group applied transcription factors, Mash1, Ngn2, Sox2, Nurr1 and Pitx3 to human fibroblasts, and found that dopamine neuron-like cells were produced directly. These cells stained positive for dopamine neuron-specific markers and took up and released radioactively-labelled dopamine, just as the control dopamine neurons. When transplanted into rat PD models, the rats’ symptoms improved, with the animals’ rotational behaviour (a measure for their motor abilities) recovering.
Of course, the reality of generating new dopamine neurons that successfully transplant into patients with PD is still far from becoming a viable clinical treatment. Nevertheless, the discovery that Liu’s mix of transcription factors is sufficient to reprogram already mature cells directly into dopamine neuron-like cells presents an exciting step forward towards treating this devastating disorder.
If you have been living on Earth recently, you’ll have come across the news that a certain Hollywood actress has undergone major preventative surgery due to the discovery of a faulty gene. The gene in question is called BRCA1 and, if mutated in a certain way, it is known to greatly increase a carrier’s chances of developing breast cancer. This incident has thrust genetic screening into the limelight – but how useful is it to know the secrets concealed within your genes?
We now have technology to take screening even further. Writer and journalist Carole Cadwalladr reports in the Guardian that whole-genome screening by Illumina is now available for just $5,000. That may seem a lot, but considering it would have cost $2.7 bn just 10 years ago, it’s a hell of a price cut. Several other companies, including 23andme and AncestryDNA are also offering to screen your genome and let you know what, if any, potential disease-causing mutations you have. Some of these scans cost as little as $99.
But do you really want to know what, if anything, is wrong with your genes? In some circumstances screening can be very useful – it can save lives. When Angelina Jolie tested positive for the BRCA1 mutation, she took the decision to have a preventative mastectomy. She hopes this will allow her to avoiding the pain of cancer and the pain her children would face watching their mother suffer; a pain she herself knows all too well. In cases like this, screening and early intervention is important because we know that a mastectomy can greatly reduce a carrier’s chances of developing the disease.
Photo: Ajsmen91, commons.wikimedia.org
But what if there is no prevention for the disease detected by the sequencing? One of the more famous examples of this is Huntington’s Disease. Huntington’s is a debilitating degenerative disorder characterised by shaky, jerky movements (called chorea) and progressive cognitive decline. It is caused by a single faulty gene, huntingtin. This gene is inherited in a dominant fashion, meaning that if one of your parents has the disease, you have at least a 50% chance of also suffering. As sufferers do not generally start to show symptoms until their 40s, they may not realise they carry this mutation until after having children – who will therefore also be at risk. It is now possible to screen people for the faulty huntingtin gene. However, there is no cure for Huntington’s. Knowing you have the gene will not help you to prevent the onset of disease; therefore do you want to know? This is a dilemma that many children of Huntington’s sufferers face. Some decide it’s best to know, especially if it will influence their choice to have children, but others would prefer not to have this time-bomb ticking over their heads.
Genome screening could allow people to adjust their lifestyle to counteract a faulty gene. For example, it is common knowledge that smoking can cause lung cancer. However, everyone also seems to have a great-aunt Gladys who smoked 90 a day and died at 102 after getting hit by a bus. On the flip side, there are people like the Record Breakers presenter Roy Castle, who died of lung cancer despite being a non-smoker. It may be that your genes determine whether you are more like Gladys or Roy. If you get your genome screened and it turns out you’re more like Roy, you could adjust your lifestyle accordingly and quit (or not start) smoking.
I’m also going to use a personal example here. If you are familiar with this blog, you may know that there is a history of Alzheimer’s Disease and dementia in both sides of my family. The cause of Alzheimer’s disease is so far not clear-cut; it appears to be a mixture of genetic and environmental factors but nothing is known for sure. One of the strongest genetic links so far is a gene called ApoE. If you have a version of the gene called ApoE4 you are at higher risk of developing Alzheimer’s. However, it does not necessarily mean that you will suffer from the disease.
Cumin Seeds Photo: Humbads, commons.wikimedia.org
So let’s say, hypothetically, that I had my genome screened and it confirmed I had the ApoE4 gene. What can I do with this information? Well, the first thing I’d probably do is panic. I’ve seen Alzheimer’s disease happen and don’t really wish to go through that. However, I am now prepared. I am at higher risk; therefore I need to try and counteract that risk. There are several methods which have been suggested to reduce the risk of Alzheimer’s disease, including eating curcumin, a spice found in curry, and keeping the brain active by doing crosswords or learning a musical instrument. I could also avoid sugary foods, as there is increasing evidence of a link between diabetes and Alzheimer’s disease. So now I’m more informed, I can happily shovel spoonfuls of chicken tikka masala into my mouth with one hand whilst playing the piano with the other and hopefully I won’t get Alzheimer’s.
But there’s another side to this. If I have the faulty gene, I will probably have inherited it from at least one of my parents. Which one? Should they get screened too? What if it’s too late for them to take preventative measures and now all they know is that at some point they might get dementia? What happens if I have children? Should they be screened? How early on do you need to start taking preventative action? What if the screen flags up another faulty gene? Or several? What if I can’t prevent a disease caused by these other faulty genes and so will have to go through life knowing that I will at some point suffer from it?
As this is a whole-genome screen, as opposed to a screen for one particular gene, it is also likely to pick up genes that you weren’t even aware you carried. Some mutations are carried silently through families, or your DNA may have become mutated another way, e.g. through smoking or exposure to UV light. Do you want to know that you may at risk of a disease you may never even have heard of? Again, good if it’s preventable (for example you discover an allergy to a medicine that you haven’t yet had to take) but if it’s not preventable, what does that leave you with? That ticking clock over your head.
The other issue here is how this type of information will be used. Illumina loads the data onto an iPhone app for you, meaning that the data must be stored somewhere. Who else has access to that information? How secure is it? Could it be possible in the future that people start demanding to know the results of genome screens for potential prime ministers to make sure they’re not going to suddenly get cancer whilst they’re supposed to be running the county? And what if health insurance companies start demanding full-genome screens before you can get a policy?
Also, new genetic links to diseases are being discovered all the time. So a screen done now may miss a genetic mutation that is flagged up in the future as being a possible cause for disease. Would you have to get screened more than once? Maybe you’ll need to be screened every few years to keep up with discoveries being made.
I feel I should point out here that the science behind this technology is amazing. The fact that it is even possible is a huge achievement and a testament to the dedication and innovation of the scientists who developed it. And it was invented to help people – to screen for faulty genes with the idea of saving lives. I have worked in a lab which has collaborated with Illumina and in doing so the lab was able to identify a new Alzheimer’s risk gene (the catchily named PCDH11X). This is all useful and helpful information. However, my worry is that the information will be exploited by other people looking for a profit, or preying on people’s fears, as unfortunately these things so often are.
A coin showing your ancestor, Charlemagne Photo: Fallschirmjäger, commons.wikimedia.org
But what about if you’re having your genome screened to discover the secrets of your ancestry? This was done recently for Prince William, and the papers excitedly claimed that “he will be the first king of England to have a genetic link to India“. However, using these services to find your ancestry may be interesting but it is not always accurate. As explained by this Sense About Science leaflet, genetic screening is not an exact science. Also, when you’re told that you are related to Charlemagne, well, so is everybody else alive today (according to an episode of QI, anyway). Most genetic ancestry screens will only go via one line – either your mother’s, through mitochondrial DNA, or your father’s, through the Y chromosome line. This leaves out an awful lot of your other potential ancestors, for example your maternal grandfather or paternal grandmother. These screens do not, and probably cannot, tell you the whole story of your ancestry.
Is it a good idea to re-open Pandora’s Box, especially if you’re just curious about your genes? Will it save millions of lives or lead to a weird state where everyone has to know exactly what disease they may or may not suffer from at a given point in time? I think, like the people at risk of Huntington’s, and like Angelina, it’s a personal choice. Some people are happier not knowing, some will want or need to know. No one should ever be forced to have their genome screened. Measures also need to be taken to make sure that this information stays personal and secure. I’m nervous about the idea that what your genes hold may become public knowledge. I personally don’t think I want to know what’s in my genes. I am already aware that I am at risk of developing Alzheimer’s, and there’s no harm in taking preventative measures anyway. I do like a good curry.
The holy grail of treating neuronal injuries is to persuade damaged neurones to regrow exactly as they were. Currently doctors lack the tools to do this, but hope is in sight in the world of nanotechnology.
Unfortunately, once nerves have suffered damage they don’t simply grow back to their original position. There are a number of reasons for this:
Inflammation gets in the way
Molecules found primarily in the mature nervous system inhibit growth
Gaps formed in nervous tissue caused by the “cleaning up” of injured cells form a barrier to growing cells
Cells fail to start regrowing
But how can nanotechnology help?
Nanotechnology is the science of the very small (on the scale of billionths of a millimetre) but it’s an enormous area of research – in many countries nanoscience is the priority for science budgeters.
Successful attempts have now been made to use nanotubules as a type of molecular scaffolding to support nerve growth. A nanotubule is a tiny (on the nanometer scale) tube-like structure – like a microscopic drinking straw. The first application of these tubes showed that, when coated with substances that encourage neuronal growth, carbon nanotubles were able to promote extension of rat embryonic nerve cells. These tiny tubes acted as a physical scaffold to guide the cells, while also providing chemical signals ‘telling’ them to grow and survive.
Nanotubes made of amino acids (the building blocks of proteins) have also been developed. These amino acids can interact directly with receptors on nerve cell membranes and have proved effective at encouraging growth and limiting the damaging effects of scar tissue. Because these are composed of naturally-occurring amino acids they are not toxic to cells and caused no inflammation or immune response in animals. This is a serious benefit, as inflammation can be very damaging in neuronal injury.
However, the unique features of nanomaterials could also be associated with unique problems. At high concentrations, some studies have found nanotubes of certain sizes to cause DNA damage, accumulation and inflammation in the lungs. Another concern is that nanoparticles can move around the body: one study showed that nanoparticles could be transmitted up nerves and into the brain. Nanotechnology may represent an exciting opportunity in medical science, but it also comes with the major challenge of understanding how the behaviour of these materials interacts with the human body.
Are you convinced that Mount Everest tastes like strawberries? Or that Friday is a deep green colour? Does hearing your friend Dave’s name make you wretch? If so, you might be entering the baffling world of synesthesia.
Synesthesia (synaesthesia in British English) is a neurological condition whereby one’s senses literally merge. It means ‘joined perception’ and can cause names to have a particular taste, letters to have a particular colour and a whole host of other sensory fusions.
It may sound more like a psychedelic experience in a drug-induced haze but this is a sober reality for a number of people. Some of the most famous creative types of our times have been diagnosed or suspected to have synesthesia. Marilyn Monroe was described by the biographer Norman Mailer to have a “displacement of the senses which others take drugs to find… she is like a lover of rock who sees vibrations when she hears sounds”.
Image credit: CaramelBeauty77
Stevie Wonder reportedly has sound-colour synesthesia whereby even though he is blind, he ‘sees’ the colour of the music. This added sensation is not restricted solely to arty types, however. Richard Feynman, the excellent Nobel Prize winning physicist, claimed “When I see equations, I see the letters in colours”, before quipping, “I wonder what the hell it must look like to the students”.
Estimates put the number of synesthetes at between 1 in 200 and 1 in 100,000 (which basically means we really don’t know how many people experience synesthesia). Some even claim it could be as high as 1 in 23! If any of this sounds familiar to you, you can test whether you may have synesthesia here.
There is a lot of fascination from scientists into this condition. The organisation of the senses is seen to play a major role in formation of memories. When you form a memory of a person, you link the information from multiple senses. The sound of their voice, the colour of their hair, the letters of their name all form your memory of that person. But for most of us, these senses still exist as separate aspects of our memory of that person. You don’t intrinsically link the letters of their name to their hair colour.
Synesthetes have secondary sensory experiences that are completely involuntary. Some synesthetes say that the colour of someone’s name is actually how they remember them. They may remember the name Dave by the colour orange more than the letters of the name.
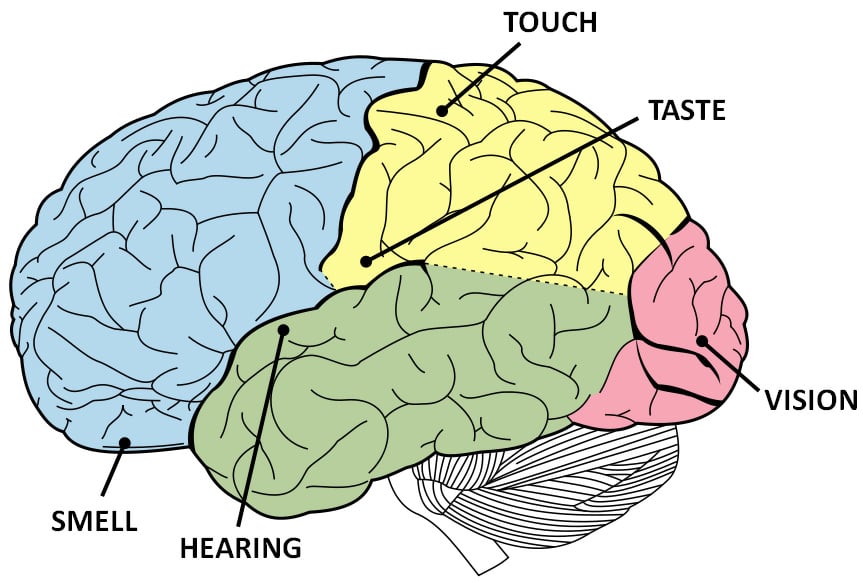
This is where the science behind it all comes in. Sensory information should be contained separately but able to be integrated at will. Different sensory information is processed in largely the same way but in distinct sensory regions. You can see below the various parts of the brain that are responsible for the different senses. As you can see they are spatially separate. The beauty of the brain is connecting this information as and when it is needed.
What appears to be the case in synesthetes is that these sensory regions are intrinsically connected. For example, sound-colour synesthetes seem to have more activity in colour-processing regions of their visual cortex (known as area V4) while listening to sounds. Instead of distinct pathways being linked at will, it could be the case that these two systems are bound together and stimulation of one sense also activates another.
It is interesting to be able to see these differences in the brains of synesthetes. What is not very clear, however, is why synesthesia is around at all. Does having synesthesia benefit you in any way? It appears that actually it might.
Synesthetes have been known to be better at remembering phone numbers, for example, suggesting they may have better memories. Letter-colour synesthetes have also shown they can be better at discriminating between different colours, whilst hearing-motion synesthetes are better at visual tasks. So could this be a rise of the superhumans – an evolutionary advantage to be able to process more sensory information than the rest of us?
Further research into synesthesia will not be a purely academic exercise but will contribute further to our understanding of the human brain. How the brain links information together on request is one of the major mysteries of neuroscience, a point focused on in Obama’s BRAIN initiative. As synesthetes show remarkable differences in how they integrate information, it will be fascinating to see whether they can be the valuable subjects to advance our knowledge of the brain.